The genetic risk factors for breast cancer to develop are age, being a female, and having a family history of the tumor. In developed countries the risk of breast cancer in women at the age of 29, 39, and 49, is, respectively, one in 2000, one in 215, and one in 50. The lifetime risk of breast cancer reaches the highest values in women 70 and older: one in eight !. In the latter age group the incidence has progressively increased in the last fifteen years as it was one in ten in 1997 and one in nine in 2003. Why is it happening? Cancer is a genetic disease but it needs some triggers to develop. There is now a good evidence that triggers of breast cancer can be found in lifestyle and environment and most probably are the followings: having fewer children and in later life; reduced breastfeeding; widespread hormone replacement therapy (administered to contrast the debilitating symptoms of the menopause); increased alcohol consumption, and excess of weight (especially after menopause). Oestrogen and other hormones are strongly implicated in breast cancer, and both pregnancy and breastfeeding reduce the amount of circulating hormone. Each birth decreases the risk of breast cancer by 7%. Every year of breastfeeding cuts the risk by 4.3%.
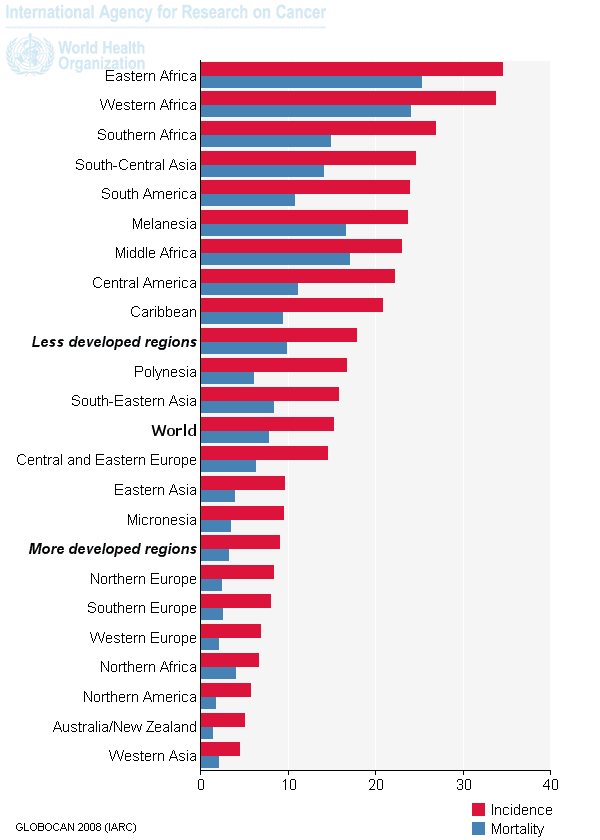
Women in developing countries have lower rates of breast cancer mainly because they start to have babies at a much younger age and have higher parity. In Sub-Saharan Africa, higher incidence rates and relative frequencies of breast cancer have been reported in association with urban than with rural residence but, in any case, the incidence of the disease is much higher among white women in Africa than among black African women. Notice that this is just the opposite of what has been reported for afroamerican women as compared to white women in the USA (see my previous post on the topic). In the future decade a progressive change in women’s lifestyle (on the model of western women) will probably take place also in many countries of the African continent and this will parallel a rise in breast cancer incidence. We should get prepared: the fight against breast cancer can be successful only if local health systems provide early diagnosis and proper treatment facilities.